Gout and it’s partner pseudogout are common causes of short bursts of joint pain. While they can affect anyone at any age they tend to affect men 40 years or over.
These two conditions are also known as ‘crystal arthropathies’ because both are caused by collections of sharp crystals in the joint. The crystals irritate the special lubricating tissue between the two bones (synovium), triggering inflammation resulting in pain, redness, and swelling in the joint.
Gout and pseudogout are usually managed by local doctors and specialists called rheumatologists. Orthopaedic surgeons can play a role in treatment of gout and pseudogout:
- Arthroscopy can be used to wash out affected joints. This is typically used for pseudogout. Alternatively, a diagnosis of gout may be under question and an arthroscopy can be performed to rule out other causes of joint pain, eg septic (infected) arthritis.
- Severe long-standing disease can cause deformity and intractable pain in the joints. The orthopaedic surgeon may be asked to replace or fuse the joint to relieve symptoms and make walking easier (see Fusion of the Large Toe).
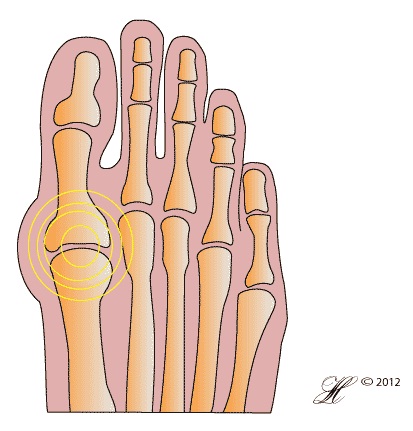
This illustration shows the swelling and pain caused by gout in it’s most common joint – the large toe (1st MTP Joint).
Symptoms
Gout and pseudogout cause intense bursts of pain:
- Sudden sharp pain, usually affecting the joint between the foot and the big toe (1st metatarsal joint). Pain often but not always begins at night.
- The affected joint is red, very swollen and warm, sore to touch and painful when moved.
- Gout most commonly affects the base of the big toe (the 1st MTP), however other joins in the foot may also be involved. Throughout the body, gout also affects the hands and wrists and rarely the larger joints.
- Pseudogout most commonly affects the knees, but can also affect the first MTP joints and other joints throughout the body.
- Gout can sometimes affect the elbow (see Olecranon bursitis).
Generally, these painful episodes last hours to days and resolve by themselves. This does not mean that the gout has gone away, but rather that crystals in the joints have dissolved temporarily.
Over time, the affected joints may become thickened and stiff. Pseudogout in particular is associated with stiffening in the knees as the crystals form a line of calcium interfering in joint function.
Causes
The reason some people develop gout and pseudogout and others do not is not always clear.
Gout is more common than pseudogout, and can affect most joints in the body, though the most common site is the at the base of the big toe (the first metatarsophalangeal joint or MTP). It is caused by collections of urate, a substance that is a normal waste product of cells in the body, but which, for a variety of reasons, builds up in the blood and then in the joint.
Risk Factors
Gout often affects older men with a history of alcohol use, but is also known to occur in people with kidney disease, those who have been treated with chemotherapy for cancer, and in people with no other medical conditions at all.
Pseudogout is associated with some conditions, like hypothyroidism, but this is a relatively weak association. There is also thought to be some genetic component, resulting in family members having increased risk of developing pseudogout.
Investigations
Gout
Gout is common, and your GP will probably be confident of the diagnosis after listening to you and looking at your foot. However, there are many other conditions with similar symptoms, so tests that may be ordered include:
- X-Rays of the foot and/or ankle. In acute attacks of gout/pseudogout X-Rays will be normal, so your doctor is ordering these tests to check for other conditions, like fractures.
- Blood tests
- More sophisticated imaging, like MRI or CT scans, are generally not necessary.
The best test for gout is a needle aspirate. This involves taking a sample of your joint fluid through a needle. The sample can then be tested and photographed to show the crystals. This is a very useful test and the best way to confirm gout, and to distinguish between gout and pseudogout.
Gout can be difficult to diagnose because it can seem similar to other conditions, including septic arthritis, haemophilic arthritis, rheumatoid arthritis and trauma including stress and compression fractures. Usually, a fine needle aspirate of the joint fluid is required to diagnose gout definitely.
Pseudogout
Like gout, pseudogout is diagnosed through needle aspiration.
Other tests that are useful include:
- X-Rays. Unlike gout, the changes of pseudogout are often visible on X-Ray. Your doctor may order knee X-Rays in addition to images of your foot/ankle as pseudoarthritis commonly affects the knees, and may be present even when you are not suffering knee pain.
- Blood tests. There are a number of extra tests your doctor may perform to check you don’t have an underlying cause for high calcium in the blood. These include:
- Thyroid and parathyroid tests
- Electrolyte levels, like calcium, magnesium and phosphorus
Complications
Complications associated with gout include:
- Joint stiffness. The most common complication of gout is the development of chronic stiffness and thickening in the affected joints.
- Kidney stones – if you have high levels of uric acid in your blood, your kidneys need to work hard to excrete the acid into your urine. Once in the urine, the uric acid can form crystals that become kidney stones.
- Gouty tophi in the ears and elbows. Uric acid from the blood collects in different areas of the body, most commonly the ears and elbows, forming hard painless lumps. It’s important to remember these lumps are not tumours and are not dangerous in and of themselves. They do however provide a storage of uric acid that can be intermittently released into your blood, causing acute attacks of gout.
- Urate nephropathy – very rarely, sufferers of gout develop kidney problems from the high levels of uric acid. This needs to be reviewed by a specialist and treated.
Complications of pseudogout include:
- Stiffening of affected joints
- Deformities
Treatment
Resting the foot and protecting the joints with soft shoes can help with pain and swelling. Sudden attacks can also be treated with:
- Colchicine – this medication is very useful in helping treat acute attacks of gout (though not pseudogout). This drug can be prescribed by your GP.
- Anti-inflammatory medications like ibuprofen. These can be bought over the counter at pharmacies.
In some cases, your doctor or surgeon may remove excess fluid from the joint through a large needle. They may also inject a local anaesthetic or steroid into the joint space to calm down the inflammation. In most cases, neither of these are necessary.
Long-term Treatment | Gout
If you have recurrent gout, your GP or rheumatologist may prescribe specialist medications:
- Probenecid – this drug helps your kidney to excrete the uric acid. While it is effective, it can increase the risk of kidney stones.
- Allopurinol – this drug stops the formation of uric acid from your cells. It is very effective and used by many people, but it can interact with other drugs and has some side effects that you should discuss with your doctor.
Pseudogout
In some people, over the counter painkillers like ibuprofen are adequate. More potent medications can be prescribed by a GP or by a rheumatologist.
Surgery
When the joints affected by gout and pseudogout are destroyed, surgery may be necessary. This tends to be either joint fusion or joint replacement. For more information, see fusion of the big toe.
Seeking Advice
Your Family Doctor (GP)
Your Family Doctor will be able to diagnose and help treat your problem. He or she will be able to
- tell you about your problem
- advise you of the best treatment methods
- prescribe you medications
- and if necessary, refer you to Specialists (Consultants) for further treatment
If you need further review, you may be seen by a rheumatologist. If you have long-standing gout affecting your kidneys, you may need to see a kidney specialist, or nephrologist.
Orthopaedic surgeons may be called to help diagnose your condition, washout your joint or correct severe deformities.
Prevention
The medications allopurinol and probenecid are designed to prevent attacks of gout. Unfortunately, there is no equivalent for pseudogout.