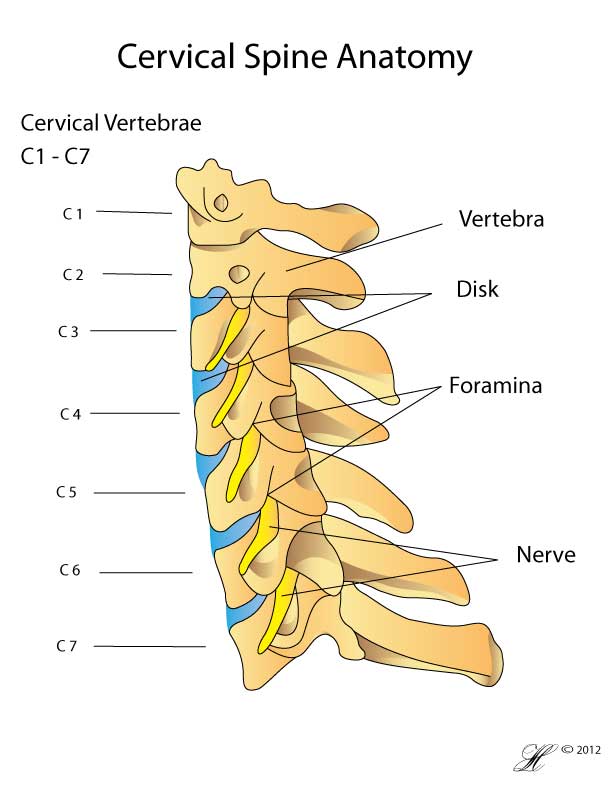
Diagram of the Cervical Spine (neck) showing normal anatomy
The term ‘whiplash’ describes a sprain of the neck causing pain. Usually this is due to a car accident, where the neck is suddenly stretched backwards as the rest of the body is forced forward. The sudden change in position strains the ligaments and muscles supporting the neck, and occasionally also causes damage to the vertebra and discs.
There are a number of symptoms of whiplash, the commonest being neck pain and stiffness, and headaches. Symptoms usually set in several hours after the initial injury. While whiplash does sometimes develop into chronic neck pain, most people see their symptoms diminish gradually over the months following the initial injury.
Whiplash can be very distressing – pain can be severe and may be complicated by numerous other symptoms. In addition, recovery is slow with residual symptoms persisting for some time. Despite this, it is important that you remain optimistic and as active as possible while caring for your neck, as the majority of whiplash sufferers recover within 12 months.
Symptoms
The symptoms of whiplash include:
- Pain:
- Pain may be felt in the neck, at the back of the head or in the shoulders and shoulder blades.
- Depending on which tissue has been damaged, the pain may be sharp or an ache.
- The pain is usually worse with movement of the neck
- Neck stiffness & decreased range of motion
- Numbness, pain or tingling in the shoulder or arm
- Headaches
- Other symptoms including visual disturbances, ringing in the ears (‘tinnitus’) and dizziness occasionally occur.
Causes
The sudden forces acting on the neck during a car accident strain the muscles, ligaments, bones and joints of the neck. The pain of whiplash is consequently thought to arise from a combination of these structures, including:
- Disc – whiplash can cause the disc cushioning the vertebral bodies to ‘slip’, or push out and compress the nearby nerve, resulting in shooting pains in the neck, shoulder or arm
- Ligaments and muscles – there are a number of long strap-like muscles and ligaments running down the neck that may be injured during whiplash. Typically, injury to these tissues causes an aching-type pain.
- Subtle fractures and injury to the spinal joints (especially the facet joints) is common in whiplash.
Risk Factors
You are at increased risk of sustaining a whiplash-type injury when:
- Your neck is already either flexed or extended when the car accident occurs
- The car accident is more serious – in general, cars that crash at greater speeds will result in more injuries to their passengers.
Investigations
Your doctor or surgeon will examine your neck and the rest of your body for any signs of nerve damage.
Other tests that your doctor may order include:
- Blood tests
- X-Rays of the neck and through the mouth.
- Sophisticated imaging like MRI scans are sometimes used
- Occasionally bone scans are used to diagnose subtle fractures.
Complications
At the time of the injury, whiplash can be associated with:
- Neurological disturbance, including vision or hearing disturbance and numbness or tingling in the shoulders and arms.
- Fractures. Subtle fractures of the cervical spine are not always immediately apparent.
Long-term complications of whiplash include chronic neck pain and headaches. Many people have only minimal pain or headache long-term, however a small number of people (around 5%) will have significant symptoms lasting more than six months, and require ongoing care.
You may be at risk of chronic pain if:
- The initial neck pain was severe
- You are elderly and have had previous neck injuries
Treatment
Whiplash can usually be treated with short-term rest and over the counter medications.
- Your doctor may prescribe a soft collar to reduce the movement of your neck. Frequently however, this is unnecessary.
- It’s important to start gently moving your neck as soon as possible. As in lower back pain, you need to keep using your neck to promote the strength and function of the muscles and speed recovery.
- Anti-inflammatory medications like ibuprofen can help reduce pain and swelling.
Your doctor or physiotherapist may then prescribe exercises to keep your neck mobile.
Treatment for Chronic Pain
Your physiotherapist will be able to show you some exercises to strengthen the muscle groups in your neck, shoulders and upper back.
While you can continue to use anti-inflammatory medications, you should check with your GP that you will not develop side-effects from prolonged use.
Your doctor or surgeon may discuss the use of injections to help control your pain. Injections of steroids (anti-inflammatories) and/or local anaesthetic can help reduce swelling, pain and irritation in the soft tissues. In the neck, the injections are usually directed into the facet or Z-joints between the vertebra.
Seeking Advice
If you have persistent neck pain and stiffness after a serious injury, like a car accident you should see your local doctor. NB if you lose consciousness at any time, you should go to the emergency department.
Your Family Doctor (GP)
Your Family Doctor will be able to diagnose and help treat your problem. He or she will be able to
- tell you about your problem
- advise you of the best treatment methods
- prescribe you medications
- and if necessary, refer you to Specialists (Consultants) for further treatment
Prevention
You can try to reduce the risk of whiplash developing into chronic pain by:
- Staying positive
- Beginning to move your neck as early as possible
F.A.Q. | Frequently Asked Questions
References
Bogduk, N., ‘The anatomy and pathophysiology of whiplash’, Clinical Biomechanics, Vol. 1, No. 2, 1986, pp 92-101.
Carroll, L., et al., ‘Course and Prognostic Factors for Neck Pain in Whiplash-Associated Disorders (WAD)’, Journal of Manipulative and Physiological Therapeutics, Vol. 32, No. 2S, Feb 2009, pp. S97-S107.
Schofferman, J., et al., ‘Chronic Whiplash and Whiplash-Associated Disorders: An Evidence-Based Approach’, Journal of American Academy of Orthopaedic Surgeons, Vol. 15, No. 10, Oct 2007, pp .